The Quiet Eligibility Crisis Coming for Medicare Dual-Eligible Members

Co-authored by Manny Felix and Nikita Singareddy
Most of the conversation about H.R. 1 has focused on work requirements. But buried in the same law is a set of changes that will hit a different population just as hard - and with far less warning: older adults and people with disabilities who rely on Medicaid, Medicare Savings Programs (MSP), and Low-Income Subsidy to afford their healthcare.
These individuals aren't focused on policy changes - they’re focused on whether they can afford their care. In the background, the infrastructure that kept them enrolled without requiring action is evolving, introducing new uncertainty and risk.
Three programs, one pipeline
To understand what's at stake, you need to know how three federal programs fit together.
Medicare is a federal program that provides health coverage for Americans 65 and older and for individuals with certain disabilities. It's not free. Medicare Part A covers hospital stays and is premium-free for most beneficiaries. Part B covers outpatient care - doctor visits, preventive care, durable medical equipment - and requires a monthly premium of $202.90 in 2026. In most cases, Medicare covers about 80% of approved medical costs, leaving beneficiaries responsible for the remaining 20%. For low-income individuals, that cost-sharing is often only manageable because of additional support through Medicaid or Medicare Advantage plans.
The Medicare Part D Low-Income Subsidy (LIS), also known as Extra Help, is a federal program administered by the Social Security Administration (SSA) that makes prescription drugs more affordable for low-income Medicare beneficiaries covering premiums and deductibles, reducing copays. For those who qualify, the impact can be life-changing, significantly decreasing out-of-pocket costs and improving access to essential medications.
Medicaid and Medicare Savings Programs (MSP) are joint federal and state programs that are essential in making Medicare affordable for low-income beneficiaries. Medicaid covers the approximate 20% coinsurance not covered by traditional Medicare, closing a critical gap in coverage for this population. Someone enrolled in both Medicare and Medicaid is what the healthcare industry calls "dual eligible”, and most receive their coverage through Dual Eligible Special Needs Plans (D-SNPs), a type of Medicare Advantage plan. MSP further supports affordability by covering monthly Medicare premiums, protecting beneficiaries from having those costs deducted from their limited Social Security income. Beneficiaries have to apply directly to these programs in their state of residence.
How the pipeline worked
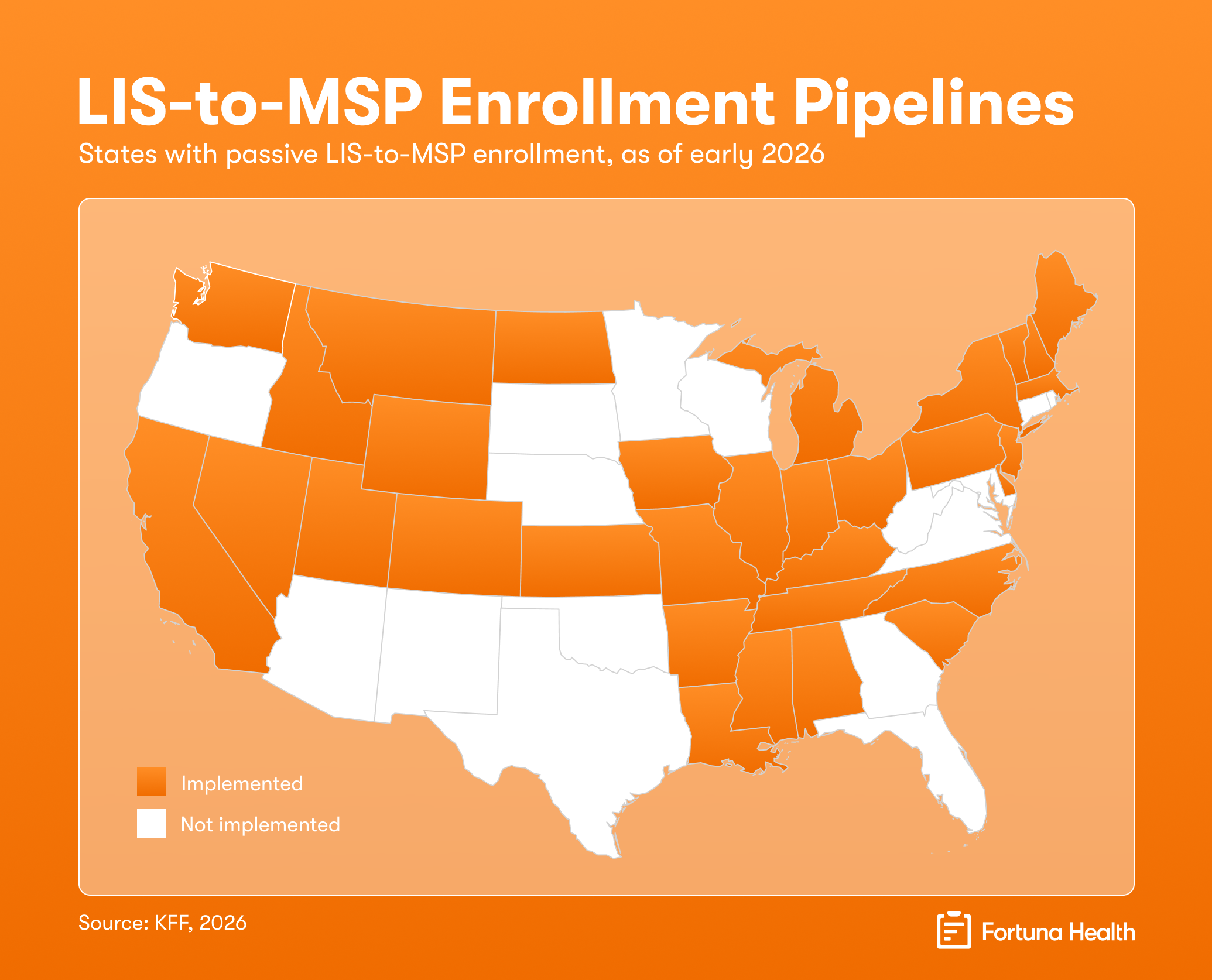
Because LIS, Medicaid, and MSP serve overlapping populations with similar eligibility criteria, a growing number of states built passive, streamlined enrollment pipeline. When SSA identifies someone as LIS-eligible, the state uses that data to automatically enroll them in Medicaid or MSP and when states identify Medicaid/MSP eligibility, beneficiaries can be seamlessly enrolled in LIS. These streamlined processes eliminate duplicative applications and ensure vulnerable individuals receive the full benefits for which they qualify.
There are roughly 12 million people enrolled in Medicaid and MSPs nationally.
The whole logic of the pipeline was simple: don't ask someone who is already proven eligible to prove it again.
But even before H.R. 1, only 56.7% of eligible beneficiaries were enrolled in Medicaid, MSPs, and LIS between 2018 and 2020 - meaning roughly 4 in 10 people who qualified never received the benefit. The passive enrollment pipeline intended to align and close that gap, but H.R. 1 is placing a 10-year pause on those efforts.
What H.R. 1 changes
H.R. 1 places a 10-year moratorium on CMS rules from 2023 that pushed states to build and maintain these passive enrollment pipelines. States that hadn't yet built the pipeline - like Rhode Island, West Virginia, and Connecticut - now face no federal pressure to do so before 2034. States that had already built one aren't required to dismantle it, but they're no longer required to maintain it either. Once it becomes discretionary, budget pressure will do the rest.
The District of Columbia was actively implementing LIS-to-MSP enrollment when H.R. 1 passed. That work has stopped.
What this means in practice
Without the passive enrollment pipeline, eligible individuals fall through the cracks. Those who qualify for Medicaid and MSP are not automatically enrolled in LIS, and vice versa. Instead, they receive a notice suggesting they may be eligible and should apply. Many don't. The result is predictable and preventable: beneficiaries lose critical assistance for prescription drugs and medical cost-sharing, exposing them to significantly higher out-of-pocket costs.
This breakdown not only undermines the purpose of these programs, but it also drives financial instability and creates avoidable barriers to care for the very populations they were designed to protect.
For managed care plans, this creates a direct financial and operational challenge. Medicare beneficiaries who lose Medicaid face higher out-of-pocket costs and may no longer be eligible to remain enrolled in a D-SNP. At the same time, those who are not enrolled in LIS may no longer be able to afford their prescription copays, which can rise to as much as 25% coinsurance.
Many Medicare beneficiaries will face higher costs through no fault of their own, increasing the risk of medication non-adherence, worsening health outcomes, and avoidable downstream costs for the healthcare system.
What health plans and states should do now
The window to get ahead of this is short. A few concrete starting points:
Know your current LIS-to-Medicaid/MSP pipeline. If your state is one of the 32 that built passive enrollment, understand how it's funded, who operates it, and whether it has continued legal and administrative support post-H.R. 1. If your state isn't one of them, understand what that gap means for your dual-eligible population today, not in 2027.
Segment your dual-eligible book by Medicaid/MSP status. LIS-eligible members who are enrolled in Medicaid/MSP are your highest-risk group. They're more likely to be confused about what they need to do, and may struggle navigating the application process without assistance.
Don't assume outreach alone solves this. A 2002 GAO review of SSA's annual outreach campaign about MSP eligibility found the campaign increased enrollment by 0.5%. The de minimis enrollment shows that the barrier isn't just awareness but the application’s confusing forms and complex documentation requirements. Effective engagement must pair with timely, proactive support.
Build the active engagement infrastructure now before coverage losses start. For states and programs that previously relied on passive enrollment, members won’t realize there’s a problem until they face higher prescription costs at the pharmacy counter. Without proactive outreach, beneficiaries may fall through the cracks, putting them at risk of skipping doses or abandoning treatment, unaware that they must complete a separate application to regain LIS. Worse, they may file complaints or disenroll and switch plans.
For states, plans, and other stakeholders, this is a moment to demonstrate what proactive support and care management actually looks like for your most vulnerable members.
If you want help thinking through how to get there, reach out to Manny Felix at Blue Cross Blue Shield of Arizona or the Fortuna Health team.
The views and opinions expressed by Manny Felix and Nikita Singareddy are their own and do not necessarily reflect those of their employers or any affiliated organizations.